Explanation:
This patient has an extrusive and lateral luxation of his primary (baby) tooth, so it can be pulled. There is no need to reinsert the tooth. He also has a laceration of the gingiva that needs to be repaired.
Epidemiology
Injuries are inevitable as children learn to crawl, walk, and run. Falling face forward puts them at risk for orofacial injuries, especially dental injuries. For children < 6 years, dental injuries account for about 20% of all physical injuries. Thankfully, at these ages, most dental injuries will be of primary teeth.
However, trauma to primary teeth can lead to the following:
- - Delayed eruption
- - Enamel hypoplasia
- - Injury to secondary teeth
- - Tooth discoloration
Pathophysiology and diagnosis
The first thing to remember is that primary teeth are lettered and adult teeth are numbered. Remembering this will save you from embarrassment if you need to consult a specialist!
The primary central incisors are E and F. These are at the highest risk of injury, given their anterior location in the mouth. This patient sustained an injury to tooth F.
Secondary (adult) teeth begin to replace primary (baby) central incisors around age 6–7. Obtaining a history from a parent may be helpful here. Knowing whether the tooth fairy has come for their child’s teeth is helpful. Injury to secondary teeth is far more concerning.
Along with tooth numbers and letters, some basic anatomy definitions may be helpful:
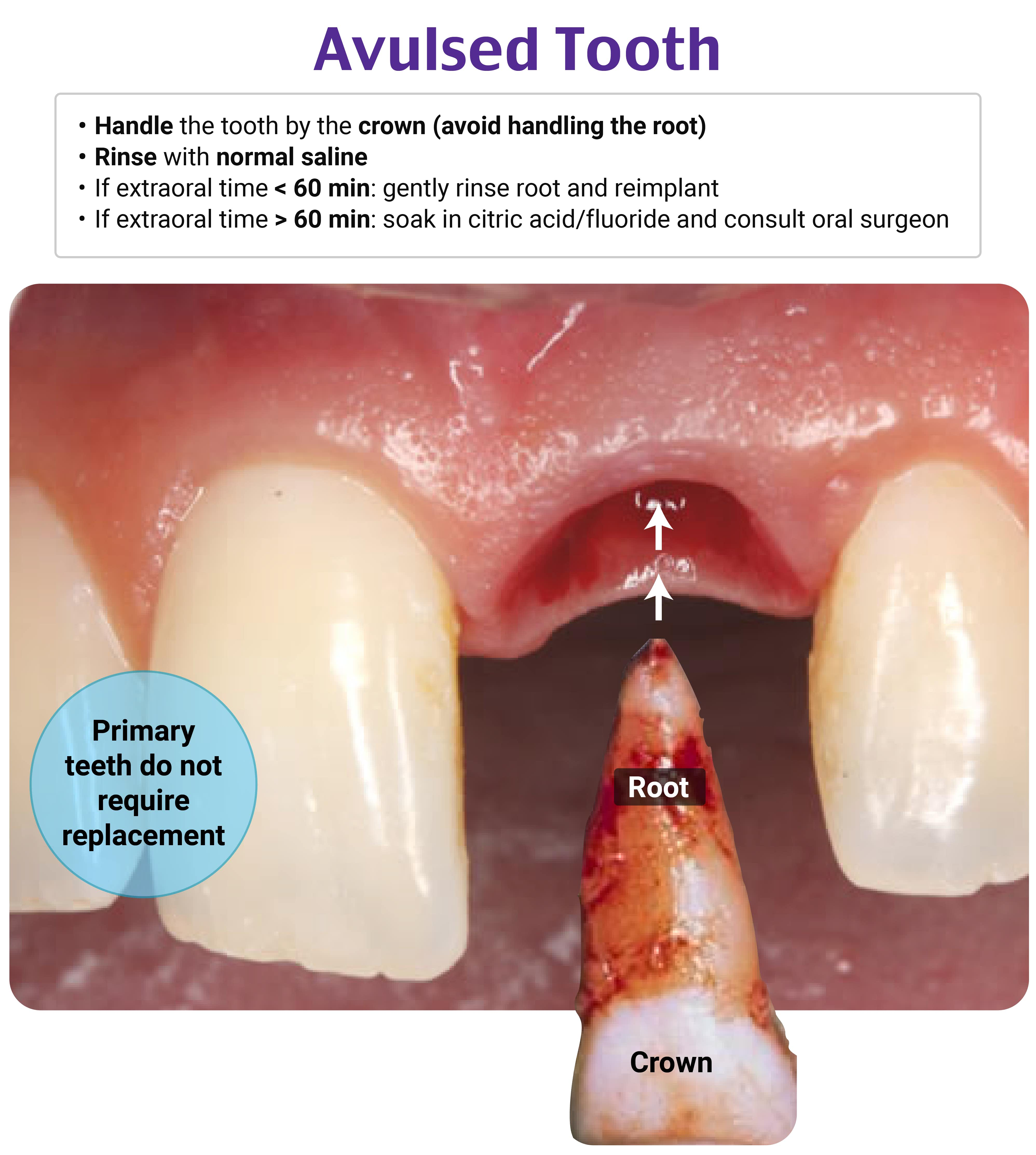
- - Dental avulsion occurs when a tooth is completely out of its socket in the alveolar bone. The patient may have swallowed it or brought it in for examination.
- - Trauma that impacts a tooth inward toward the alveolar bone is a dental intrusion. The tooth will appear shorter than its neighbors.
- - Dental extrusion occurs when a tooth is displaced out of its socket. The tooth will appear elongated. It is highly mobile, as it is held intact by only a few gingival fibers.
- - A lateral luxation of the tooth involves a horizontal force that displaces the apex of the tooth toward the lip. The tooth will be displaced and immobile. Fracture of the alveolar process is present.
Dental X-rays are not widely available in most EDs. If these are available, periapical or occlusive X-rays can identify a widened periodontal ligament space.
Treatment
Following up with a dentist in the morning is a good idea but is not the best next step.
A good first step is to consult your local dentist. They can provide helpful advice on treatment and follow-up recommendations. A pediatric dentist was consulted in this situation. Extracting the tooth from the adjoining tissue (because it was a primary tooth) and repairing any gingival lacerations was recommended. Reinsertion would be recommended for secondary teeth.
A dental block will provide anesthesia and allow for a better exam. A supraperiosteal (also known as periapical) or an anterior superior alveolar nerve block can be used for patients with incisor injuries.
Pediatric (and adult) patients may be scared or anxious about a needle coming toward them.
Intranasal sedatives such as midazolam are a good adjunct to facilitate the dental block.
Steps to performing a supraperiosteal nerve block:
- - Consider intranasal sedation
- - Apply a topical anesthetic over the gingiva of the desired tooth
- - Obtain a 25-gauge needle, 3 cc syringe, and 1–2 cc of 1% lidocaine*
- - Aim the needle toward the root of the desired tooth
- - Inject 1–2 cc in the mucobuccal fold (where gingiva meets buccal mucosa) above the tooth
- *This is a small amount, but it’s always good to calculate the toxic dose in all patients, especially pediatric patients
This patient was a real champ and did not require any sedation! He received a supraperiosteal nerve block with successful analgesia. A scalpel was used to loosen the tooth away from overlying tissue. The tooth did not need to be placed in saline-soaked gauze, milk, or a balanced salt solution, as it was not going to be reinserted. He had a gingival laceration that was repaired with one absorbable suture. His completed exam is shown below.

References:
- Day PF, Flores MT, O’Connell AC, et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 3. Injuries in the primary dentition. Dent Traumatol. 2020;36(4):343–359. https://www.aapd.org/media/policies_guidelines/e_injuries.pdf
- Goswami M, Aggarwal T. Prevalence of traumatic dental injuries among 1- to 14-year-old children: a retrospective study. Int J Clin Pediatr Dent. 2021;14(4):467–470. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8585904
P.S. Want to test your knowledge with more questions like this? Take advantage of 15% off the Rosh Review Scholar EM Qbank. You'll get 25 new questions with detailed explanations + images and 50 CME annually!

Use code: RebelEMScholar